
It felt like it took forever to get to that first day. We started building Concentric in Spring 2019, but the ideas, prototypes and previous iterations have been around much longer. At times I felt as though we were in a computer game, where each ‘Approval’ along the journey was a ‘Boss level’ but I was never quite sure if that was the final one or whether there was another boss lurking around the corner, as yet unknown to us.
We all remember how quickly things changed in March 2020. From our perspective we were inches away from finalising our first integration, ready to go live, and could see the coronavirus pandemic accelerating at pace towards us. It was becoming increasingly clear that at any moment it could gobble up the IT resource we were dependent on to get over the line. Somehow, with probably only a day to spare, we got there and in April ‘20 we launched our first pilot.
In truth the first couple of weeks were as soft a pilot as you could imagine. Concentric co-founder Ed would guide on the ground within the department, and was doing most of the consent conversations within the department anyway. But using software for real will always highlight issues and niggles, and make visible areas and stakeholders somehow not considered during user testing.
What had been planned as a small pilot - couple of specialties for a few months - quickly changed in May ‘20. With teams fighting to keep urgent cancer services going, we were bombarded with clinicians - day after day and both from that initial NHS Trust and elsewhere - having shifted to remote consultations and remote pre-operative pathways asking “Can Concentric help me with remote consent?” Thankfully the answer - after a quick shift in product priorities a month earlier - was yes!
12 months later we’re used at 5 UK NHS Trusts / Health Boards - at a range of volumes from digital consent by default and across all specialties (including non-surgical specialties such as oncology, cardiology and neurology) through to deployments across a handful of specialties. Concentric is also used at a number of UK private clinics and hospitals, and a couple of sites outside the UK.
Here’s what use has looked like, per week, over the first year (note that big dip in activity during the 2nd national lockdown):
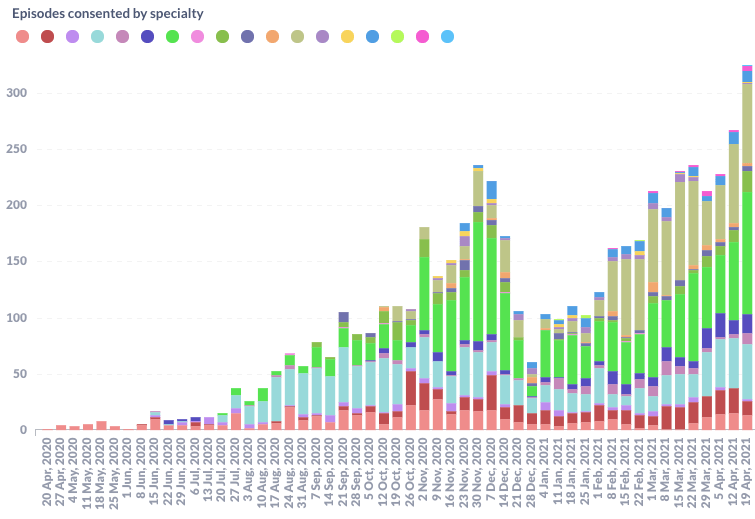
For our hospital deployments we’ve seen a number of different models being used, and we’ve worked with some fantastic project and clinical leads who have championed the shift to digital consent every day. With pandemic restrictions limiting our ability as a team to be on site, that local leadership has made the world of difference. Thank you!
Things we’re proud of
In many ways the last 12 months have been accompanied with a somewhat surreal feeling for me. What had been a bedroom project for Ed, Martyn and I since 2013, was finally - thanks to grant funding and support from lots of people along the way - becoming a reality. Actual people were using our actual product.
The next question was whether they liked it, and whether it was having an impact - both from a patient and clinician perspective. Not being there on the ground definitely made it more difficult to get a good sense of how the change was going down, so it was with some nervousness that I waited for the results of the first large scale evaluation sent out to clinicians in Autumn ‘20 - no-one wants to hear that they’ve got an ugly baby after all. Clinicians responded overwhelmingly that they felt Concentric was improving the consent process, reducing their admin time, and strikingly each one of them would support its procurement and use across the Trust. Sigh of relief!
Patients get asked for their feedback on the Concentric consent process, by their healthcare organisation, a couple of weeks after treatment, and over a thousand patients have by now responded to that survey, giving an average of 9/10 for their experience. Most patients’ free-text comments relate to their appreciation of having easy access to their personalised information:
Really good information, and nice to be able to read it at leisure, and in the depth I want, and discuss it with relatives.
Whilst some make us smile in their simplicity:
It appears to be both necessary and useful for both patient and surgeon
We’ve tackled some tough challenges over the past year. Medicine is complex, and often messy. Historically, health technology, as we all know, has often led to an even more complex mess.
Solving the challenge of combined procedures/treatments was always one that I knew we needed to get right if Concentric could really be loved by clinicians, and was the thing that I’d seen other teams trying to crack the consent problem do really badly. No-one wants to present a patient with 5 different generic leaflets for their “Rigid cystoscopy + bladder biopsy +/- TURBT +/- retrograde pyelogram +/- ureteric stent insertion” and have to explain that most of the information doesn’t relate to their individual circumstance but sorry it’s the best that’s available.
Combined procedures really stole our attention for a number of months, but hopefully most would agree it’s made a huge difference; I’m now far more confident that Concentric can thrive in the complex and messy clinical world. Thanks to the team, especially Jon and Martyn for the enthusiasm in coming back to this particular challenge every morning for those weeks! Here’s a 2 minute clip of how building a combined procedure works and what that translates into for our patients:
Another thing that has been very noticeable has been the speed with which we’ve been able to integrate with different systems at each organisation, ensuring that clinicians can search the patient database, and automatically send completed consent forms back into the main electronic health record (EHR). Whilst we’re still a way away from the promised land of internet facing FHIR API’s at each organisation, I’ve been pleased to see that all of our deployments have been Cloud deployments. With integrations connecting systems within NHS networks out to Concentric’s cloud, data is where clinicians need it to be, essentially instantly, and right within their workflow. Where others talk of 6-12 months of integration work, we talk of 4-6 weeks - even faster if FHIR, and that’s a very different conversation to have with Trusts in terms of delivering impact within weeks.
Our mission statement talks of transforming how we make decisions about our health. Over the next couple of years we’ll increasingly explore how a digital consent process can be a vehicle for change, especially in the shared decision making (SDM) space. We weren’t sure whether Concentric in its current form would be having a significant impact on SDM, but an academic evaluation seems to be suggesting it is - more on that when published.
What our data shows
Those who know us will know that we’re an inquisitive bunch trying to bring human and data insights together to deliver something really great. Whilst there are a number of upcoming publications exploring in detail the insights from the use of Concentric, I thought it would be interesting to share a few at a high level.
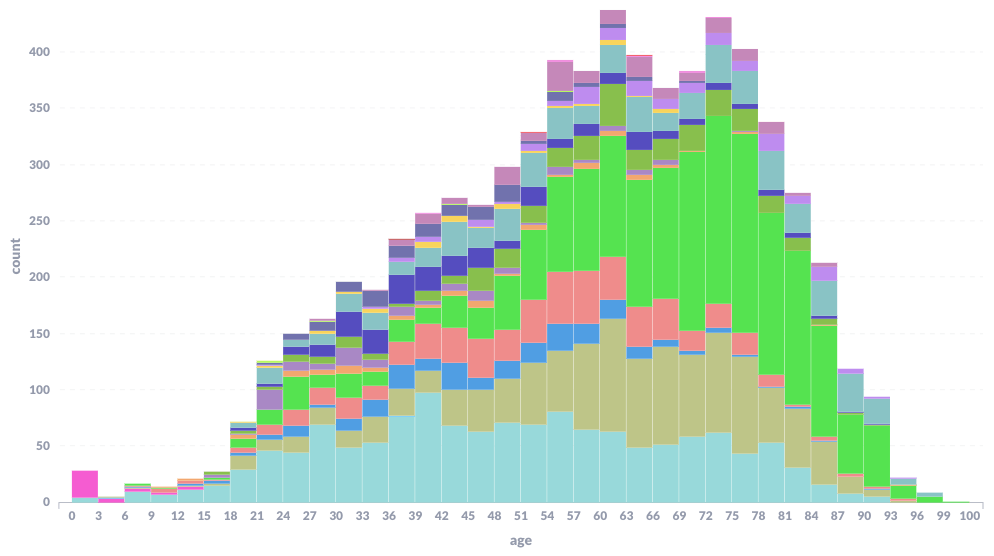
We often get asked, can digital consent be used by all ages. The answer is absolutely yes, with some patients engaging mostly remotely, and others preferring to be supported to engage with Concentric with their clinician.
Here’s a histogram of patient age, from our youngest patient at 0 (Consent Form 2 obviously!) through to our oldest at over 100! Each colour is a different specialty, you can see the skew within some specialties such as ophthalmology (bright green).
Over the past couple of years, the legal and ethical standpoint against day of surgery/treatment consent - unless absolutely necessary - has become clearer, but we can tell that this remains a widespread practice. There is more work to do to really understand what our Concentric data shows us - particularly relating to the quality of any consent conversation that may have been had prior to what looks like a ‘day of surgery’ Concentric consent. However, I think we can be reasonably confident that for around 1 in 2 patients, a significant amount of new consent information, and documentation of consent, is happening on the day of treatment. There is significant variation here between different organisations, types of organisation, and specialties within an organisation.
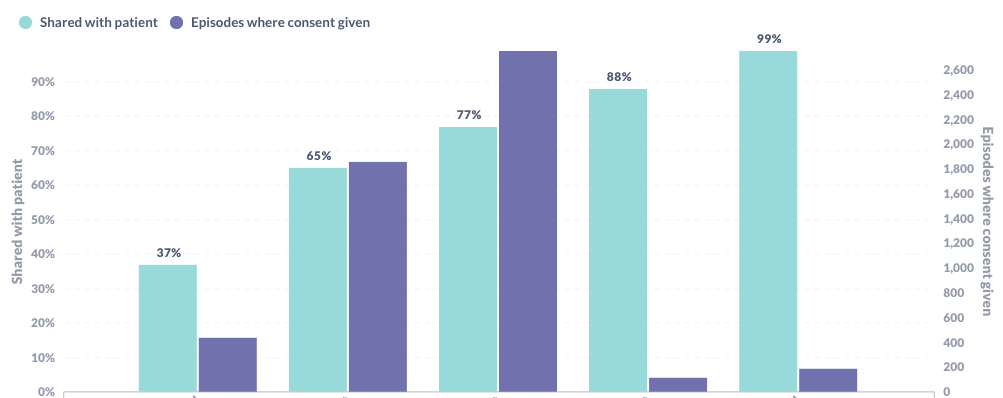
A fundamental premise of Concentric is that patients have access to their personalised, evidence-based information. One of the barriers to this is accessibility of contact details for patients. 12 months ago clinicians needed to enter a patient’s email address to share a secure link, and that was definitely enough of a barrier (as well as typos when entering) for a significant number of patients not to receive their information. By now in the majority of cases either or both an email address and mobile number come through integration, meaning that sharing with patients is the default. Of note - at most organisations mobile numbers are more commonly recorded than email addresses, so when we turned on our SMS functionality a couple of weeks ago we saw another increase in sharing. Here’s the rate of sharing at a few Concentric organisations over the last 12 months, showing the variation, with a notable reduction in the rate of sharing at one non-integrated deployment.
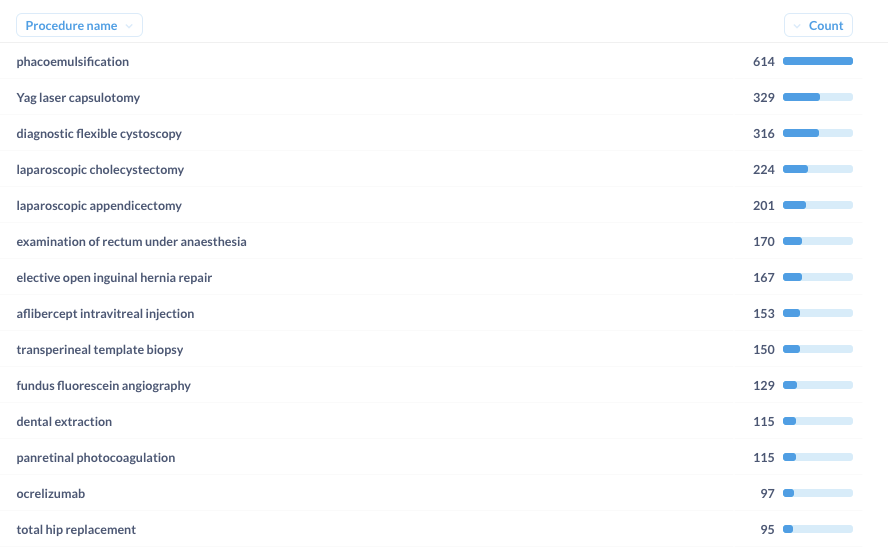
To be able to be used as the default method of consent across an organisation, across all specialties, it stands to reason that a digital consent application needs a lot of content. Concentric has evidence-based, curated templates for over a 1000 different procedures and treatments within its structured database (what we call the Concentric Ontology). The vast majority of the time, it’s a fraction of that content that is used. Of the 500 templates that have been used over the course of the first 12 months, only the below 12 have been used 90+ times, before getting into a long tail of rarely used content. (Of course it’s important that the content is there when you need it, no-one wants to be switching between paper and digital depending on what’s on the operating list that day)
Our next 12 months
Our principal aim over the next 12 months is to continue improving the product every week (those of you who use Concentric will have noticed that every couple of weeks little improvements get released. This is not a product - like so many others we are used to in healthcare - that stays the same and never gets better). And we’ll add new functionality such as language translations. By focussing on the product we hope to see that graph of use continuing to rise exponentially, both in the UK and internationally.
Much of our strength is down to how close we are to our users, and as we grow over the coming months I’d like to use this opportunity to reaffirm to you that we don’t want that to change. We want to hear your niggles, feel any frustrations, and fix them with you. One of the emails I received this week said “sorry, I asked you to bleep me in my last email, I forgot you’re not based at …, woops!” - but that’s exactly how close we want us to feel, and continue to be over the next 12 months and beyond.
Thank you to everyone for all of your support and guidance, and as ever please do reach out to find out more or if there’s something we can be doing better. Daf